

Background
Premature death from opioid-related causes imposes an enormous public health burden across the United States. Between 2001 and 2016, the number of opioid-related deaths in the United States increased by 345%, from 9489 to 42 245 deaths (33.3 to 130.7 deaths per million population. Moreover, opioids may have immunosuppressive properties independent of their psychotropic effects; opioid use has been associated with increased invasive pneumococcal disease in a nested case-control study of 1233 Medicaid patients from Tennessee. In liver transplant recipients, opioid use disorder has been associated with increased mortality after transplant. The impact of opioid use disorder on patients receiving blood and marrow transplant (BMT) remains to be defined.
Methods
We performed a retrospective analysis of all consecutive adult patients who had BMT (autologous and allogeneic) from 1/1/2008 through 1/1/2018 at the James Comprehensive Cancer Center. Overall survival (OS) was measured from the date of transplant to the date of death, censoring at date of last follow up if alive. Progression free survival (PFS) was measured from the date of transplant to the date of disease progression or the date of death, whichever occurred first, censoring at last follow up if no event. OS and PFS were estimated by the Kaplan-Meier method and compared using the log-rank test. Opioid use (OU) was defined as a binary yes/no variable if an opioid was prescribed upon discharge from the hospital after BMT. The impact of OU, along with other patient, disease, and BMT related factors, on PFS/OS, was analyzed using Cox regression method.
Results
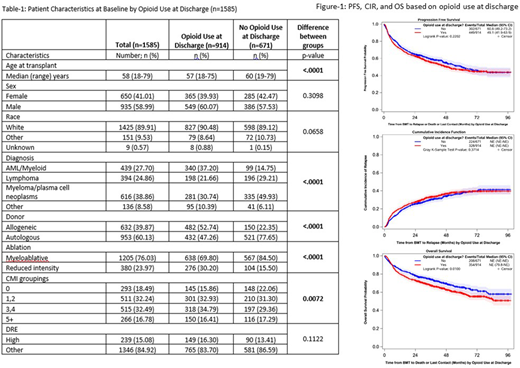
A total of 1585 patients were included in the analysis (Table 1). The median age at BMT was 58 (range=18-79) years; 59% were males; 60% had autologous transplants; and 58% were prescribed opioids upon discharge from the hospital. OU was significantly more in patients who were younger, have had allogeneic transplant, reduced intensity conditioning, had acute myeloid leukemia (AML), or higher BMT comorbidity index (CMI). On univariable analysis, OU was not associated with cumulative incidence of relapse (CIR) or PFS however it was associated with inferior OS; hazard ratio (HR)=1.25, 95% CI: 1.06-1.49; p=0.01 (Figure-1). There were no differences in CIR, PFS, or OS when autologous and allogeneic transplants were analyzed separately. Upon multivariable analysis of OS, OU lost statistical significance after controlling for age, diagnosis, type of transplant, intensity of conditioning regimen, CMI, and disease risk index (DRE). Of interest, OU independently predicted for superior OS at 100 days and 365 days post-BMT; HR=0.29, 95% CI 0.16-0.50 (p=<.0001) and HR=0.47, 95% CI 0.32-0.69 (p<0.001); respectively.
Conclusion:
Our results suggest that opioid use (OU) may have a long term negative impact on survival in BMT patients. The apparently protective effects of OU early on after BMT is elusive but may be possibly related immunomodulatory effects of opioids. A major limitation of our study is that OU is analyzed at a single time point at hospital discharge after BMT. We plan to undertake a more detailed analysis of ongoing OU after discharge and its impact on survival outcomes after BMT.
Brammer:Celgene Corporation: Research Funding; Seattle Genetics, Inc.: Speakers Bureau. Efebera:Celgene: Research Funding; Ohio State University: Current Employment; Pharmacyclics: Research Funding; Takeda: Honoraria, Speakers Bureau. Mims:Abbvie: Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Other: Data Safety Monitoring Board; Syndax Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees; Kura Oncology: Membership on an entity's Board of Directors or advisory committees; Leukemia and Lymphoma Society: Other: Senior Medical Director for Beat AML Study; Agios: Consultancy; Novartis: Speakers Bureau. Chaudhry:Sanofi: Consultancy, Membership on an entity's Board of Directors or advisory committees. Bumma:Sanofi: Speakers Bureau; Amgen: Speakers Bureau. Khan:Amgen: Consultancy; Janssen: Consultancy. Devarakonda:Janssen: Consultancy. Jaglowski:Novartis: Consultancy, Research Funding; CRISPR: Consultancy; Juno: Consultancy; Kite, a Gilead Company: Consultancy, Research Funding. William:Kyowa Kirin: Consultancy, Honoraria; Merck: Research Funding; Seattle Genetics: Research Funding; Incyte: Research Funding; Guidepoint Global: Consultancy; Dova: Research Funding; Celgene: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal